Inside the Brain Circuit That Keeps OCD Going
OCD is not really an anxiety disorder in the traditional sense, but rather a disorder of a brain circuit that cannot properly stop.

One of the strangest things about OCD is that you can know perfectly well that a thought makes no sense, or that an action has already been completed, and yet still be unable to leave it alone.
For example, you know the door is probably locked or that your hands are clean. You also understand that another hour of analysing a memory won’t produce any further certainty - but the brain doesn’t seem to register that completion. No matter how many times you repeat the action, something still feels very wrong.
That gap between knowing and stopping is one reason that makes the neuroscience of OCD so important. You see, OCD is often largely described as an anxiety disorder. And indeed, anxiety is clearly a part of it - sometimes an overwhelming part. But anxiety alone does not explain the repetitive thoughts, the rigid behavioural patterns, the persistent error signals, or the sustained feeling that an action remains unfinished.
Rather, a more useful biological framework is that OCD involves a failure of regulation in a set of connected brain loops known as the cortico-striato-thalamo-cortical circuit, or CSTC circuit (Milad & Rauch, 2012; Pauls et al., 2014).
(And yes, it is a terrible name for an extraordinarily important system.)
That CSTC model has become the dominant neurobiological framework for OCD because evidence from brain imaging, neuropsychology, lesion studies, genetics, animal models and neuromodulation repeatedly points towards abnormalities in these circuits (Milad & Rauch, 2012; Pauls et al., 2014). However, despite that convergence, we must note that it remains just a model rather than a complete explanation for the emergent phenomena.
That’s because OCD does not live in one neat loop, and no single scan can diagnose it. In fact, the real biology is far messier, more distributed and almost certainly differentiable between patients. And this is exactly what a very important paper on ‘Regional, functional and transcriptomic decoding of multidimensional brain structure alterations in obsessive-compulsive disorder’ has just revealed in Nature Communications (Cardoso Saraiva et al., 2026).
The circuit that decides what happens next
The CSTC circuit connects four broad components.
First, the cortex - particularly frontal areas of the brain - which represents goals, expected outcomes, possible threats and the significance of what is happening.
Second, the striatum (part of the basal ganglia) that helps select which thoughts, actions or behavioural programmes should be allowed through.
Third, the internal globus pallidus and substantia nigra, which act as major output structures of the basal ganglia. They regulate the thalamus, largely through inhibitory signalling.
And fourth, the thalamus, which sends information back to the cortex and helps to reinforce, update or sustain the selected programme.
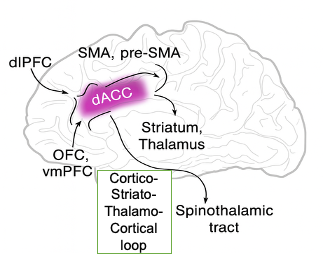
As implied by the above, this is not a single circuit but a family of partly overlapping loops as different frontal regions connect with different parts of the striatum and thalamus (Milad & Rauch, 2012; Pauls et al., 2014). Among these frontal regions, the orbitofrontal cortex, or OFC, evaluates outcomes, rewards, punishments and whether circumstances have changed. The anterior cingulate cortex, or ACC, is involved in conflict monitoring, effort and error signalling. The supplementary motor area (or SMA) and pre-supplementary motor area help prepare and control actions, while the dorsolateral prefrontal cortex supports flexible, goal-directed control.
And together, these regions help answer basic questions that the brain must resolve constantly. Namely, is this important? What should I do? Did the action work? Should I continue, switch or stop?
In OCD, that system seems to have become biased towards continued processing, whereby a possible error is treated as unresolved; a possible threat remains salient; an action that should terminate is selected to go again.
But this does not mean the person literally chooses the compulsion. In fact, quite the opposite is true. The problem is that the circuitry involved in choosing and stopping behaviour is no longer producing a reliable sense of completion.
I’ve actually had people asking me why their partner just can’t stop these compulsive behaviours - taking it personally, as though their partner with OCD is intentionally choosing the compulsions over them. But that’s completely the wrong way of looking at it because the person with OCD is not choosing the compulsions. In fact, they are likely to hate these compulsions and would give anything to make them stop.
The problem is that they just can’t.
The direct, indirect and hyperdirect pathways
The basal ganglia are sometimes described using an accelerator-and-brake analogy.
The direct pathway helps facilitate a selected thought or action. The cortex sends an excitatory glutamate signal into the striatum. Striatal neurons then inhibit the basal ganglia’s output nuclei. And because those output nuclei normally inhibit the thalamus, inhibiting them releases the thalamus from restraint.
This is called disinhibition, which is the act of removing an inhibition. The result is that the selected action or cognitive programme is more easily reinforced through the thalamus and back into the cortex. In simplified terms, the direct pathway says allow this through.
In comparison, the indirect pathway does almost the opposite. It runs from the striatum through the external globus pallidus and subthalamic nucleus before reaching the basal ganglia output structures. Its overall effect is to increase inhibition of the thalamus, and in simpler terms, it says to suppress the competing programmes.
Then there is the hyperdirect pathway, which runs rapidly from the cortex to the subthalamic nucleus without first passing through the striatum. It can impose a fast, broad interruption of activity while the brain decides what to do next. And because of this, it is sometimes described as an emergency brake (Nambu et al., 2002).
Yet these pathways don’t operate as three independent switches. Instead, they work together dynamically. When you begin an action, the brain has to facilitate the chosen response, suppress alternatives and retain the ability to stop quickly when circumstances change.
The older CSTC theory of OCD proposed that the direct pathway was overactive relative to the indirect pathway. This would excessively disinhibit the thalamus, feeding activity back into the cortex and creating a self-reinforcing loop. Such a line of enquiry remains an influential hypothesis, as it fits the repetitive quality of OCD rather well. That is, once a thought or action programme gains access to the loop, it may become unusually difficult to suppress or replace.
But the simple “direct pathway too strong, indirect pathway too weak” account is no longer sufficient (Milad & Rauch, 2012). Modern basal-ganglia neuroscience shows that both pathways can be active during action, their roles varying across different striatal territories, and the timing and coordination between pathways may matter as much as their overall activity.
The deeper problem may, therefore, be poor control of action selection. That is, insufficient discrimination between useful and maladaptive responses, abnormal stopping, excessive reinforcement of habits and failure to update when an outcome has already been achieved.
The brain’s error signal that refuses to switch off
The anterior cingulate cortex (ACC) is particularly interesting in OCD. Consequently, it’s also a brain region that is a focus of ours at Serenatis Bio because of our work with Prof Trevor Robbins and his team at the University of Cambridge.
You see, when we make a mistake, the brain generates a rapid electrical response called the error-related negativity, or ERN for short. It can be measured using EEG within milliseconds of an incorrect response being made and is strongly associated with performance-monitoring systems involving the ACC.
Across many studies, people with OCD tend to show an enlarged ERN (Riesel, 2019). The brain appears to produce a stronger-than-normal error signal, sometimes even when the mistake is trivial, thereby “overblowing” events and triggering compulsive behaviours to correct the perceived mistake. That’s not to say the ERN causes OCD. Rather it may be a vulnerability marker, a consequence of illness, or part of a wider trait involving excessive performance monitoring (Riesel, 2019).
But it maps surprisingly well onto the lived experience of the disorder - anyone with OCD will recognise this ‘OCD feeling’ that something is horribly wrong and you need to check it over and over again. But even then, it still feels wrong and that’s because the internal error system continues to report that there’s a problem.
The same logic may even apply to experiences that feel “not quite right”. But in this instance, the issue is not always fear in the conventional sense. Sometimes it is an intolerable sense of incompleteness, whereby the action has not landed correctly, the thought has not been resolved, or the sequence has not reached its proper endpoint.
Research also implicates the supplementary motor area (SMA), which is involved in preparing actions. EEG measurements such as the readiness potential may help capture excessive motor preparation or difficulty inhibiting a prepared response. Early work linking ERN and readiness-potential measures with glutamate-to-GABA ratios by Prof Robbins and his group is especially fascinating, as it could help develop these as biomarkers for clinical trials (Biria et al., 2023) – something we are very interested in at Serenatis Bio for our glutamate modulator drug.
Glutamate, dopamine and serotonin
The CSTC circuit is largely built from glutamatergic connections. Glutamate is the brain’s principal excitatory neurotransmitter - carrying signals from the cortex into the striatum, from the subthalamic nucleus into basal-ganglia output regions, and from the thalamus back to the cortex.
This makes glutamate central to the circuit’s operation.
Studies using magnetic resonance spectroscopy, cerebrospinal fluid, genetics and animal models have produced evidence of altered glutamatergic function in OCD (Pittenger et al., 2011). For example, studies by our scientific advisor Prof Robbins have reported relationships between glutamate:GABA ratios in the ACC and SMA and compulsivity and symptom severity (Biria et al., 2023).
For me, the most credible hypothesis is one of poorly regulated excitatory signalling within these particular circuits. Glutamate works in balance with GABA, the brain’s main inhibitory transmitter, so circuit dysfunction could arise from excessive excitation, inadequate inhibition, altered receptor function, abnormal synaptic plasticity or a combination of these.
Comparatively, dopamine helps regulate the balance between basal-ganglia pathways. D1 and D2 receptors are strongly associated with the direct and indirect pathways respectively, although the biology is more complex than that shorthand suggests. Dopamine also influences motivation, learning, cognitive flexibility and the tendency to repeat actions that have previously reduced distress.
This may help explain why dopamine-modulating antipsychotics can augment SSRIs in some patients, while also producing substantial side effects and helping only a minority of cases (Bloch et al., 2006).
Serotonin clearly matters, too. SSRIs are evidence-based treatments, and serotonin affects cortical, striatal, thalamic and amygdala function. But their efficacy does not establish that OCD is fundamentally caused by a serotonin deficiency. In fact, SSRIs probably alter circuit dynamics and plasticity over time rather than simply correcting a missing chemical.
The important point is that these neurotransmitters do not operate in separate worlds. Serotonin and dopamine modulate a circuit whose fast excitatory signalling is largely glutamatergic.
The CSTC circuit is not the whole brain
The classic model sometimes makes OCD look too tidy. But, clearly, there are other regions involved as well (Pauls et al., 2014).
For instance, the amygdala contributes to threat learning and emotional salience. It may help explain why certain intrusive thoughts feel so urgent and dangerous, even when the person knows rationally that the threat is improbable and unlikely.
The insula processes internal bodily states, disgust, uncertainty and subjective feelings of wrongness. It has been repeatedly implicated in symptom-provocation studies, although results vary between symptom dimensions and patient groups.
The cerebellum, once treated mainly as a motor structure, is increasingly recognised as contributing to prediction, timing, error correction and cognitive regulation. Structural and functional differences have also been reported in OCD, but we still do not fully understand their significance.
The hippocampus, parietal cortex, default-mode network and broader salience and executive-control networks are similarly involved (Pauls et al., 2014).
While the CSTC framework is very useful because it provides an anatomical backbone, the reality is more likely that OCD is a problem of interaction between multiple circuits involved in threat, habit, valuation, error detection, internal sensation and behavioural control.
Why this circuit framing matters
Calling OCD a circuit disorder is not just a different description - it changes how we develop treatments.
For drug development in particular, it moves the field beyond searching for another serotonergic medicine, as it opens rational approaches involving glutamate receptors, cortical dopamine, inhibitory signalling, synaptic plasticity and other mechanisms that regulate specific circuit functions (Pittenger et al., 2011).
For biomarkers, it gives us measurable candidates: ERN, readiness potential, brain connectivity, task performance, MRS neurochemistry and perhaps genetic or computational markers (Riesel, 2019; Biria et al., 2023). None are ready to diagnose OCD in routine practice, but combinations of them may eventually help identify biologically distinct patient groups or demonstrate whether a drug is actually changing the intended circuit.
For neuromodulation, the logic is even more direct. Deep-brain stimulation, transcranial magnetic stimulation and emerging approaches such as focused ultrasound all act on nodes or pathways within these networks. Their effects provide some of the strongest causal evidence that altering circuit activity can affect severe OCD symptoms, although outcomes vary and the mechanisms remain only partly understood (Nuttin et al., 1999; Karas et al., 2019). I’ve met people with extreme OCD who have had deep brain stimulation, and the results have been remarkable. For some, their OCD has literally vanished, while for others it has reduced so significantly that they can still live a near-normal life.
But the strategic insight is simple: once OCD is understood as a failure of circuit regulation - of selecting, evaluating and stopping thoughts and actions - the therapeutic possibilities widen. It is true that SSRIs will remain an important element within the treatment pathway, but the circuit disorder description points towards therapies that are designed to act more directly on the biology that keeps the loop running.
Sources:
Biria, M., Banca, P., Healy, M.P. et al. Cortical glutamate and GABA are related to compulsive behaviour in individuals with obsessive compulsive disorder and healthy controls. Nat Commun 14, 3324 (2023). https://doi.org/10.1038/s41467-023-38695-z
Bloch, M., Landeros-Weisenberger, A., Kelmendi, B. et al. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol Psychiatry 11, 622–632 (2006). https://doi.org/10.1038/sj.mp.4001823
Cardoso Saraiva, L., Sato, J.R., Sebenius, I. et al. Regional, functional and transcriptomic decoding of multidimensional brain structure alterations in obsessive-compulsive disorder. Nat Commun (2026). https://doi.org/10.1038/s41467-026-74153-2
Karas P.J., Lee S., Jimenez-Shahed J., Goodman W.K., Viswanathan A. and Sheth S. A. Deep Brain Stimulation for Obsessive Compulsive Disorder: Evolution of Surgical Stimulation Target Parallels Changing Model of Dysfunctional Brain Circuits. Front. Neurosci (2019). 12:998. https://doi.org/10.3389/fnins.2018.00998
Milad, M. R., & Rauch, S. L. Obsessive-compulsive disorder: Beyond segregated cortico-striatal pathways. Trends in Cognitive Sciences (2012). 16(1), 43–51. https://doi.org/10.1016/j.tics.2011.11.003
Nambu, A., Tokuno, H., & Takada, M. (2002). Functional significance of the cortico-subthalamo-pallidal ‘hyperdirect’ pathway. Neuroscience Research, 43(2), 111–117. https://doi.org/10.1016/S0168-0102(02)00027-5
Nuttin, B., Cosyns, P., Demeulemeester, H., Gybels, J., & Meyerson, B. (1999). Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet, 354(9189), 1526. https://doi.org/10.1016/S0140-6736(99)02376-4
Pauls, D., Abramovitch, A., Rauch, S. et al. Obsessive–compulsive disorder: an integrative genetic and neurobiological perspective. Nat Rev Neurosci 15, 410–424 (2014). https://doi.org/10.1038/nrn3746
Pittenger, C., Bloch, M. H., & Williams, K. (2011). Glutamate abnormalities in obsessive compulsive disorder: Neurobiology, pathophysiology, and treatment. Pharmacology & Therapeutics, 132(3), 314–332. https://doi.org/10.1016/j.pharmthera.2011.09.006
Riesel, A. (2019). The erring brain: Error-related negativity as an endophenotype for OCD — A review and meta-analysis. Psychophysiology, 56(4), e13348. https://doi.org/10.1111/psyp.13348